Polycystic ovary syndrome (PCOS) is the most common cause of infertility in women between the ages of 14 and 40, which involves the association of reproductive disorders with menstrual cycle irregularities, sterility, excessive hairiness and obesity. Recent studies demonstrate the existence of a link between insulin resistance responsible for the appearance of metabolic syndrome and polycystic ovary syndrome (PCOS).
What causes polycystic ovaries?
Polycystic ovary syndrome – symptoms
Treatment of polycystic ovaries
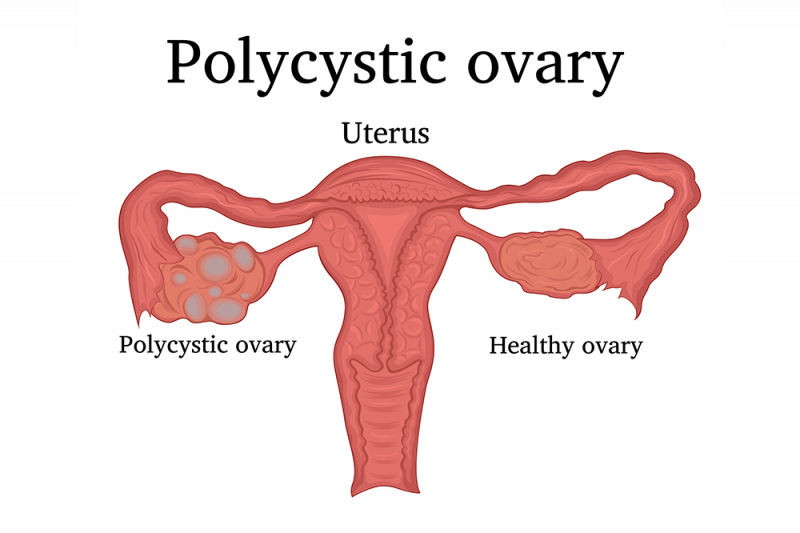
What are polycystic ovaries?
Ovarian cysts are small fluid sacs, small in size (less than 1 cm), which develop on the surface of the ovaries. Polycystic ovary syndrome implies the presence of a large number of such liquid formations.
What causes polycystic ovaries?
The causes that determine the occurrence of PCOS are multifactorial and involve genetic predisposition, specific environmental factors and endocrine disorders represented by the increase in the level of androgenic hormones and insulin (insulin causes inflammation that stimulates the ovarian production of androgenic hormones), but ovarian dysfunction is the main reason for polycystic ovary syndrome.
Polycystic ovary syndrome – symptoms
Polycystic ovary syndrome (PCOS) is clinically manifested by the following symptoms:
- Irregularities of the menstrual cycle with the occurrence of menstruation at intervals greater than 35 days
- Fertility problems
- Acne
- Hirsutism – hyperpilosity with androgynous disposition on the face, arms, anterior and posterior chest, abdomen
- Overweight
- Androgynous alopecia – hair loss in specific areas of the scalp
- Acanthosis nigricans – dark coloration of the integuments at axillary, inguinal, submammary and cervical levels
- Depression, anxiety
- Pelvic pains
- DISORDERS
- Sleep disorders
- A study published in the European Journal of Preventive Cardiology claims that certain symptoms of PCOS are present only during the reproductive years
Also, the pregnancies of patients with polycystic ovaries can present a complicated evolution with the appearance of gestational diabetes, hypertension, spontaneous abortion or premature birth.
Diagnosis of PCOS
The diagnosis of polycystic ovary syndrome is established by the gynecologist based on the anamnesis and clinical examination of the patient, but also on imaging investigations and laboratory analyses.
The laboratory analyses used to diagnose PCOS have as their main purpose the exclusion of other endocrine pathologies that can cause the occurrence of menstrual disorders and hyperandrogenism and assume:
- Determination of thyroid hormones-TSH, free T4
- ACTH stimulation test
- Determination of 17 hydroxyprogesterone and urinary free cortisol (to rule out adrenal gland disorders)
- Testosterone and anti-Mullerian hormone frequently show increased values in PCOS patients, while SHBG (sex hormone binding globulin) can have low values
- Imaging investigations represented by transabdominal ultrasound, transvaginal ultrasound and nuclear magnetic resonance of the pelvis (pelvis MRI) show the presence of immature ovarian follicles (more than 12 immature follicles) with a diameter between 9 and 12 mm and an ovarian volume > 10 cm3
Treatment of polycystic ovaries
The treatment of PCOS is complex, the multitude of therapeutic options being given by the patient’s preference to have a pregnancy in the future, but also by the associated comorbidities.
The hygienic-dietetic regime represents a form of non-drug treatment of polycystic ovary syndrome and includes a food plan that corresponds to the energy needs of the patient so that she reaches a body mass index between 18-25. Practicing regular physical activity, together with an adequate diet, contributes to the loss of excess body weight and improves the quality of life of PCOS patients.
Drug treatment includes oral antidiabetics to decrease insulin resistance and sensitize tissues to its action, as well as the secondary decrease of testosterone levels with favoring ovulation.
Oral contraceptives have the role of decreasing FSH (follicle-stimulating hormone), LH (luteinizing hormone), free testosterone and dehydroepiandrosterone sulfate and the simultaneous increase of SHBG, being used in the case of patients who do not want a pregnancy in the near future.
Ovulation stimulators are indicated for women planning a pregnancy, the treatment having the maximum success rate when it is preceded by the administration of oral contraceptives for a short period of time in order to decrease the luteinizing hormone and the risk of spontaneous abortion.
Ovarian drilling is the surgical treatment option for people with polycystic ovary syndrome and involves performing a laparoscopic intervention to stimulate ovulation through the controlled perforation of the thickened ovarian cortex with the help of a laser.
PCOS complications
The inability of the ovaries to release eggs at regular intervals causes difficulties in obtaining a pregnancy. Many patients receive the diagnosis of polycystic ovary syndrome after medical investigations are carried out to elucidate the reasons why they cannot get pregnant.
But, untreated, over time, PCOS seriously alters the quality of life of women, and especially overweight women can develop severe health problems, such as:
- Diabetes – according to the Centers for Disease Control and Prevention (USA), more than half of women with PCOS end up developing type 2 diabetes by age 40
- Gestational diabetes – diabetes during pregnancy involves risks on both sides, for mother and fetus, from spontaneous abortion, to fetal macrosomia and to obesity and diabetes in the child over the course of life
- Heart disease – as women age, polycystic ovaries are at a 19% increased risk of cardiovascular disease, according to a study published in the European Journal of Preventive Cardiology
- High blood pressure (HTN) – HTN is in turn a significant risk factor for the occurrence of serious diseases such as heart attacks, vascular accidents
- High level of LDL cholesterol and low level of HDL cholesterol – read more about LDL and HDL cholesterol | Risks and treatment of high cholesterol
- Obstructive sleep apnea syndrome – causes breathing to stop during sleep and increases the risk of heart disease and type 2 diabetes
- Cerebrovascular accident (AVC) – caused by the clogging of blood vessels and the possibility of the appearance of blood clots that lead to the occurrence of a cerebral stroke
Considering the causes that determine the appearance of polycystic ovary syndrome, the medical condition cannot be prevented.
If you are faced with menstrual cycle irregularities, fertility problems, pelvic pain or any of the previously mentioned symptoms, contact your specialist doctor for a specialist consultation.
References:
- PCOS (Polycystic Ovary Syndrome) and Diabetes, Centers for Disease Control and Prevention – https://www.cdc.gov/diabetes/basics/pcos.html
- Polycystic Ovary Syndrome (PCOS): Arguably the Most Common Endocrinopathy Is Associated with Significant Morbidity in Women – https://academic.oup.com/jcem/article/84/6/1897/2864436?login=true
- Prevalence of polycystic ovary syndrome (PCOS) in first-degree relatives of patients with PCOS – https://www.fertstert.org/article/S0015-0282(00)01662-9/pdf
- The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report – https://www.sciencedirect.com/science/article/abs/pii/S0015028208013927